Quantitative electroencephalography (qEEG) is a method of recording and analysing the electrical activity produced by the brain. It has been used in clinical neurology since the 1920s, when German psychiatrist Hans Berger first demonstrated that electrical potentials could be measured from the human scalp. Modern qEEG builds on this foundation by applying digital signal processing techniques to extract precise frequency-domain information from raw EEG recordings.
Electrode placement and the 10-20 system
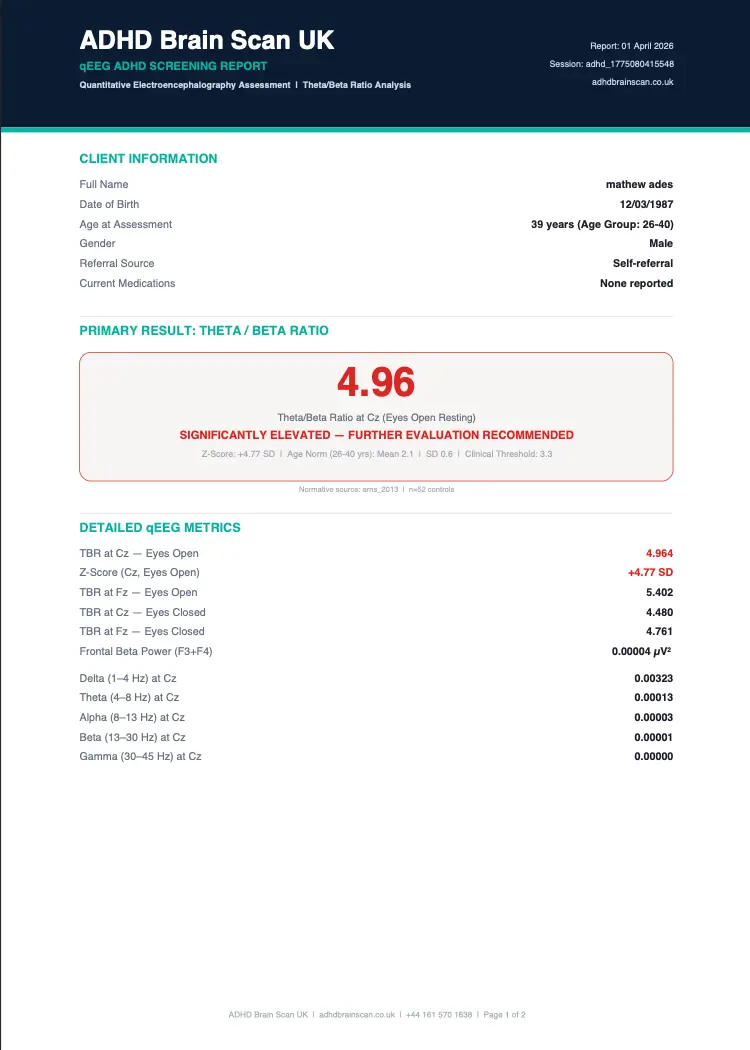
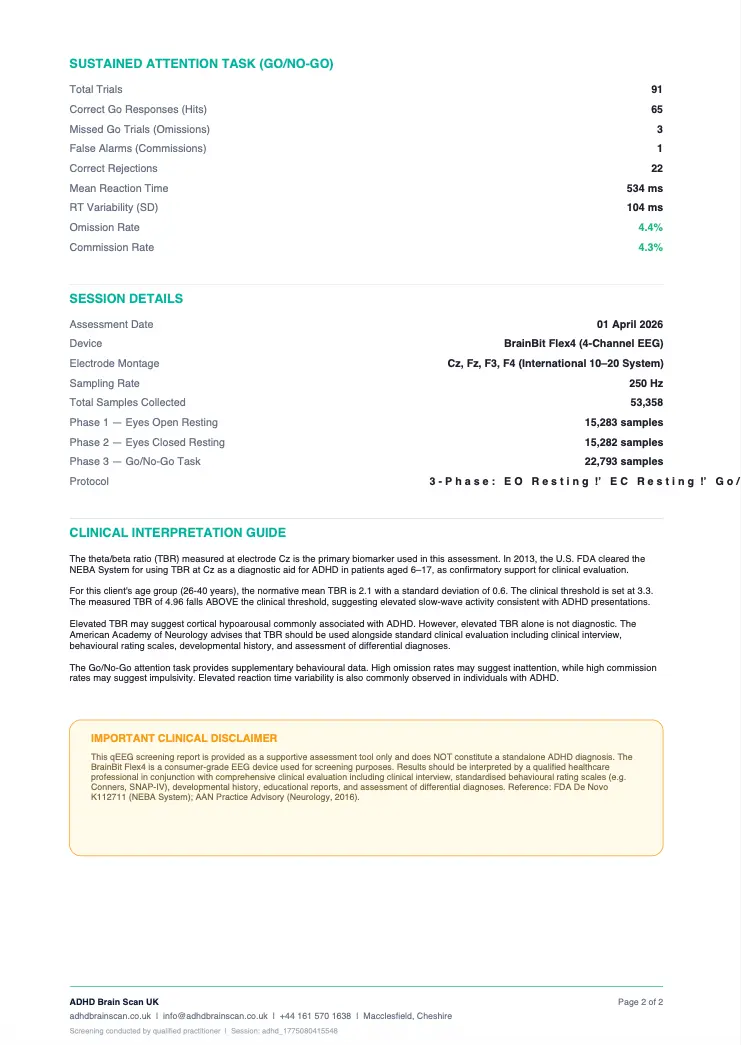
Our screening uses four electrode sites positioned according to the international 10-20 system, a standardised method for placing EEG electrodes that ensures consistent measurement locations across different subjects and sessions. The primary sites are Cz (central midline, at the vertex of the scalp) and Fz (frontal midline, above the forehead), with supplementary recordings at F3 (left frontal) and F4 (right frontal). Electrode Cz is the critical measurement point — this is the exact site specified in the FDA's NEBA System clearance and the site used in the majority of published ADHD TBR research. The frontal sites provide additional data on executive function regions and help identify lateralised differences in cortical arousal.
Signal acquisition and processing
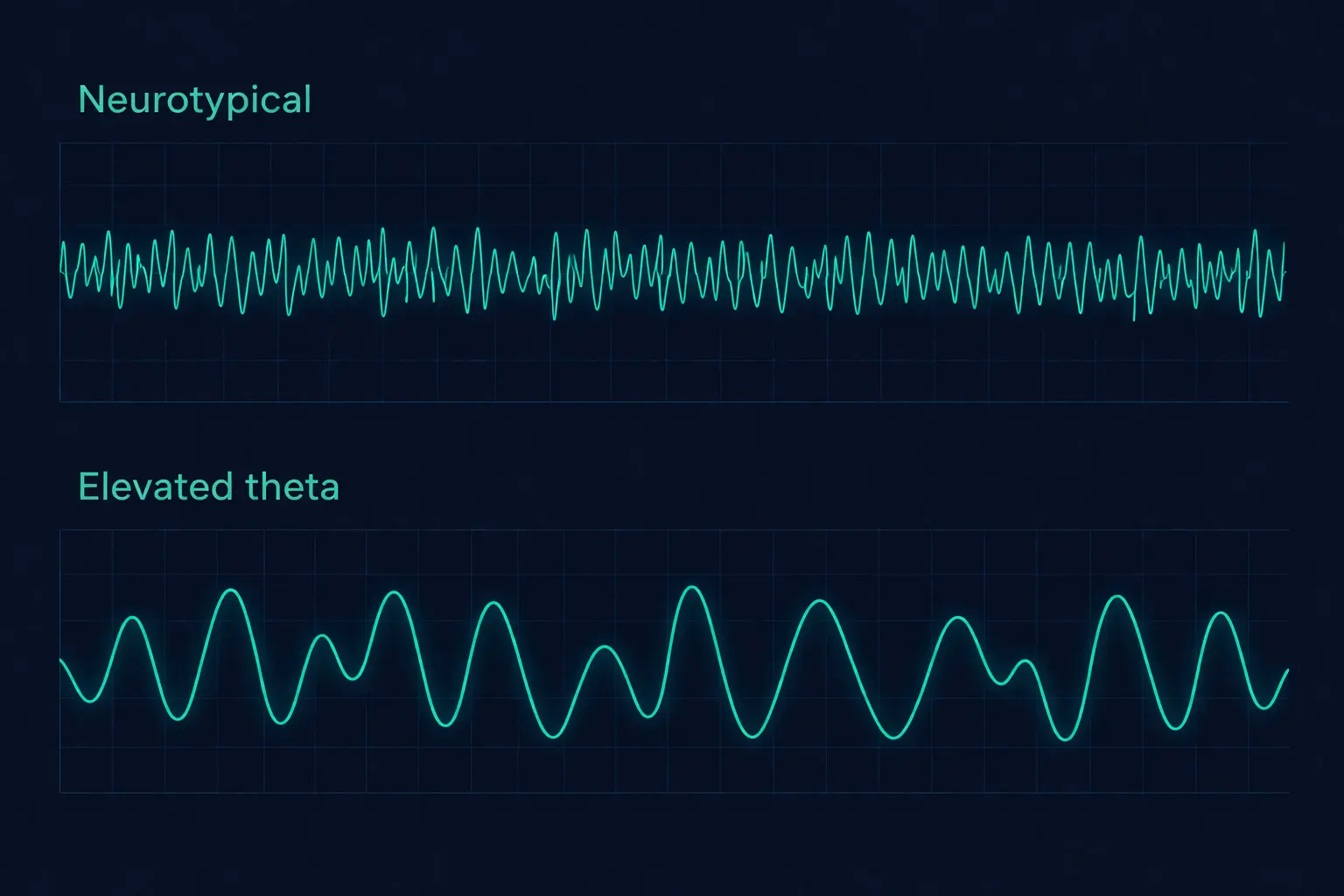
The electrodes detect microvolt-level electrical potentials generated by synchronised neuronal activity in the cerebral cortex. These raw signals are amplified, digitised at a sampling rate sufficient to capture frequencies up to 45 Hz, and then processed using Fast Fourier Transform (FFT) analysis. The FFT decomposes the complex raw EEG signal into its constituent frequency components, revealing how much power (measured in microvolts squared per hertz) is present at each frequency. This is analogous to splitting white light through a prism to reveal its component colours — except instead of colours, we see the relative contributions of delta, theta, alpha, beta, and gamma frequency bands.
Artifact rejection and quality control
Raw EEG data contains artifacts from sources other than brain activity, including eye blinks, muscle tension, jaw clenching, and electrical interference. Our processing pipeline identifies and removes these artifacts before computing the final frequency analysis. This is critical because muscle artifacts can artificially inflate beta power, and eye movement artifacts can contaminate frontal recordings. Each recording undergoes visual inspection and automated artifact rejection to ensure the computed theta/beta ratio reflects genuine cortical activity rather than noise. We also monitor impedance (the electrical contact quality between electrode and scalp) throughout the recording to ensure signal quality meets clinical standards.
The neuroscience of ADHD: dopamine and the prefrontal cortex
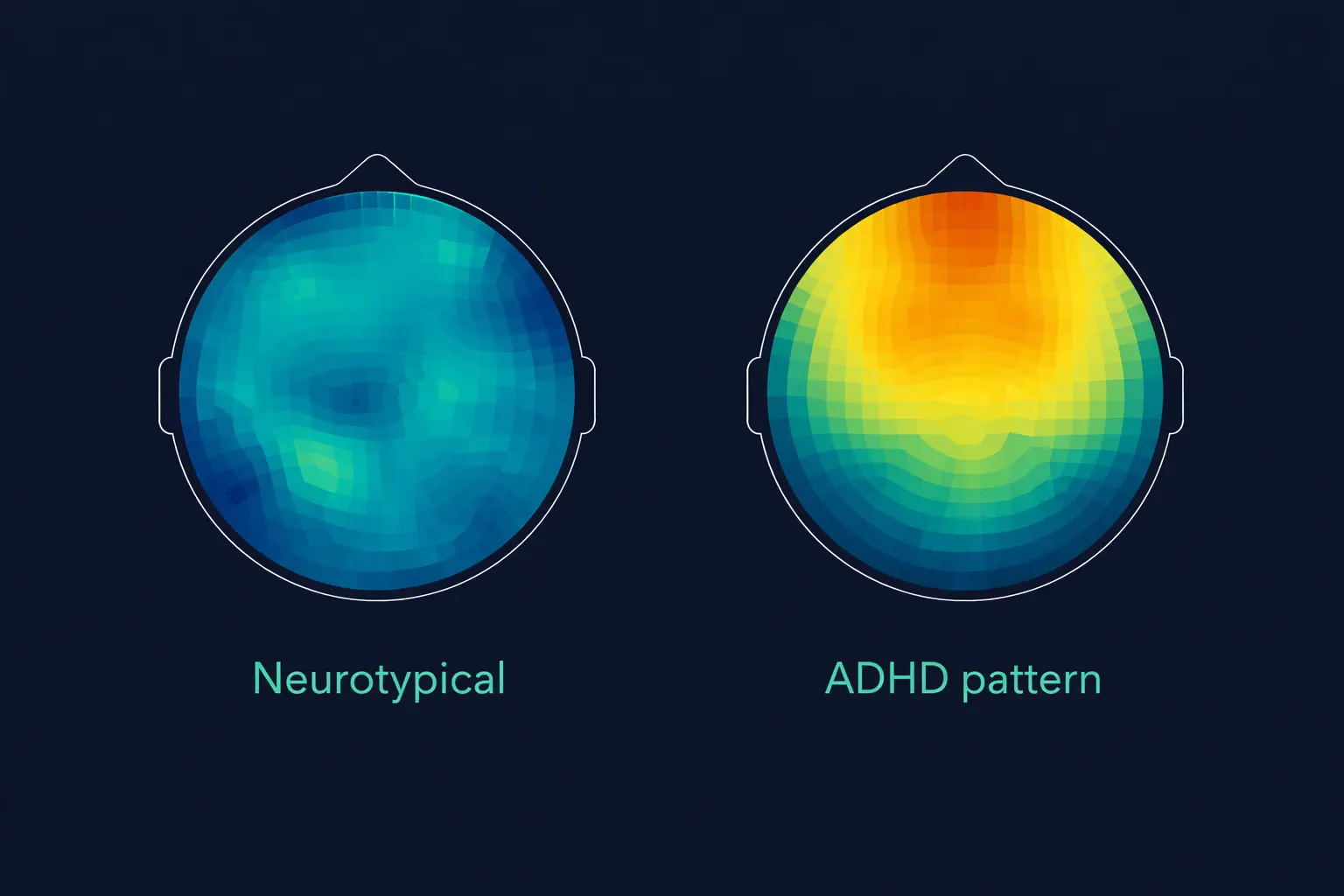
The cortical hypoarousal pattern measured by qEEG reflects underlying neurochemical differences in the ADHD brain. Research from neuroimaging and pharmacological studies has established that ADHD involves dysregulation of the dopaminergic and noradrenergic neurotransmitter systems, particularly in the prefrontal cortex and its connections to the basal ganglia and cerebellum. Dopamine plays a critical role in sustaining attention, filtering irrelevant stimuli, maintaining motivation for non-rewarding tasks, and regulating executive function. In ADHD, dopamine signalling in the prefrontal cortex is believed to be insufficient, leading to reduced cortical arousal that manifests as elevated slow-wave (theta) activity on EEG.
This dopamine hypothesis explains several key observations. First, it explains why stimulant medications (methylphenidate, lisdexamfetamine) are effective in ADHD — they increase dopamine availability in the prefrontal cortex, raising cortical arousal to more typical levels. Second, it explains why the theta/beta ratio tends to normalise when effective medication is taken, something we can objectively measure with a pre/post medication comparison scan. Third, it explains why individuals with ADHD often perform well on tasks that are inherently stimulating or novel (which naturally increase dopamine) but struggle with routine, repetitive, or low-reward tasks (which do not). The qEEG captures this prefrontal arousal state directly, providing a neurological snapshot that complements the behavioural observations made during clinical assessment.
Norepinephrine, the second key neurotransmitter implicated in ADHD, regulates alertness and the brain's signal-to-noise ratio — its ability to distinguish important stimuli from background noise. Reduced noradrenergic function contributes to the distractibility and difficulty filtering irrelevant information that characterises ADHD. Medications like atomoxetine and guanfacine target this system specifically. While qEEG cannot directly measure neurotransmitter levels, the cortical arousal patterns it detects are the downstream consequence of these neurochemical differences, making the theta/beta ratio an indirect but reliable indicator of the underlying neurobiology. For a full overview of UK medication options, see our ADHD medication guide.