Understanding Your ADHD Brain — Why It Works Differently and Why That Matters
ADHD is not a personality flaw, a character defect or a lack of willpower. It is a neurodevelopmental condition — a measurable difference in how the brain is wired, how it develops, and how it manages the chemicals that control attention, motivation and emotion. Understanding what is happening inside your brain is the foundation for everything else: effective strategies, informed medication decisions, and the self-compassion to stop blaming yourself for things your brain is genuinely struggling to do.
This page explains the neuroscience of ADHD in plain English — no jargon walls, no oversimplifications. You will understand why you can hyperfocus on a video game for six hours but cannot start a 10-minute email.
In this guide
- The prefrontal cortex — your brain’s project manager
- Dopamine and norepinephrine — the chemicals that drive focus
- Executive function — the 6 skills ADHD affects
- Working memory — your brain’s sticky note
- The default mode network — why your mind wanders
- Emotional regulation — why feelings hit harder
- The reward system — why motivation is context-dependent
- How qEEG measures your brain activity
- The theta/beta connection — what your screening measured
- Brain development — the 3-year delay
- How medication changes the brain
- Neuroplasticity — your brain can change
- The ADHD brain in women
- ADHD and intelligence — they are not related
- Frequently asked questions
The prefrontal cortex — your brain’s project manager
The prefrontal cortex (PFC) sits behind your forehead and is the most recently evolved part of the human brain. It is responsible for the things we think of as “adulting”: planning ahead, organising information, controlling impulses, maintaining focus, managing time, and regulating emotions. Neuroscientists call these abilities executive functions.
In ADHD, imaging studies consistently show that the prefrontal cortex activates more weakly during tasks that require sustained attention and behavioural control. It is not damaged or broken — it is underactivated. It needs more neurochemical fuel to reach the operating level that other brains achieve automatically.
Think of it this way
Imagine your prefrontal cortex is a project manager in an office. In most brains, this manager shows up early, stays focused, and keeps everything on track. In the ADHD brain, the manager is equally capable — but they are perpetually undersupplied. Their coffee machine is broken, their email is patchy, and their office lights keep flickering. They can do the job, but they need external support to do it consistently. That support comes from strategies, medication, or both.
Dopamine and norepinephrine — the chemicals that drive focus
The prefrontal cortex runs on two key neurotransmitters: dopamine and norepinephrine. In ADHD, the signalling of both is suboptimal — not necessarily “low” in absolute terms, but dysregulated in how they are released, received and recycled.
Dopamine — your motivation signal
Dopamine helps your brain answer the question: “Is this worth my effort?” When dopamine signalling is optimal, you can push through a boring but necessary task because your brain connects present effort to future reward. When signalling is suboptimal — as it is in the ADHD prefrontal cortex — the brain struggles to generate that motivational bridge. This is why task initiation is so difficult for tasks that are not inherently interesting.
Research shows that people with ADHD often have a higher density of dopamine transporters (DAT) — the proteins that remove dopamine from the synapse. More transporters means dopamine is cleared faster, reducing its availability exactly where the prefrontal cortex needs it most.
Norepinephrine — your alertness signal
Norepinephrine supports alertness, signal detection, and the ability to filter relevant information from background noise. It helps your brain decide what to pay attention to and what to ignore. Suboptimal norepinephrine function contributes to the distractibility and inconsistent alertness that define much of the ADHD experience.
Executive function — the 6 skills ADHD affects
Executive function is the umbrella term for the cognitive skills managed by the prefrontal cortex. ADHD affects all of them to varying degrees:
- Working memory — holding information in mind while using it (see next section)
- Inhibition — stopping yourself from acting on impulse. Blurting out comments, interrupting conversations, making impulsive purchases, sending emails you regret — these all reflect impaired inhibition
- Cognitive flexibility — shifting between tasks or perspectives. Getting “stuck” on one approach, difficulty adapting to change, or struggling to see another person’s viewpoint
- Planning and organisation — sequencing steps, estimating time, prioritising tasks. This is why a messy desk, missed deadlines and chaotic filing systems are so common in ADHD
- Self-monitoring — observing your own behaviour and adjusting. Difficulty recognising when you are going off-track, talking too much, or missing social cues
- Emotional regulation — managing the intensity and duration of emotional reactions (see below)
Think of it this way
Executive function is like a conductor leading an orchestra. Each musician (brain region) can play their instrument perfectly. But without the conductor keeping everyone in time, coordinating entries and adjusting volume, the music falls apart. In ADHD, the conductor is present but their baton keeps cutting out. The musicians are fine — the coordination is impaired.
Working memory — your brain’s sticky note
Working memory is the ability to hold information in your mind while you are using it. It is what lets you remember a phone number long enough to dial it, follow a set of spoken instructions, or keep track of what someone just said in a conversation while formulating your response.
In ADHD, working memory capacity is measurably reduced. This manifests as:
- Walking into a room and forgetting why you went there
- Losing track of what you were saying mid-sentence
- Re-reading the same paragraph five times without absorbing it
- Forgetting tasks the moment someone asks you something else
- Difficulty following multi-step instructions without writing them down
The practical response is to externalise everything. Lists, calendars, reminders, notes, alarms — these are not crutches. They are compensations for a genuine neurological difference, no different from wearing glasses for poor eyesight. See our digital tools guide for specific recommendations.
The default mode network — why your mind wanders
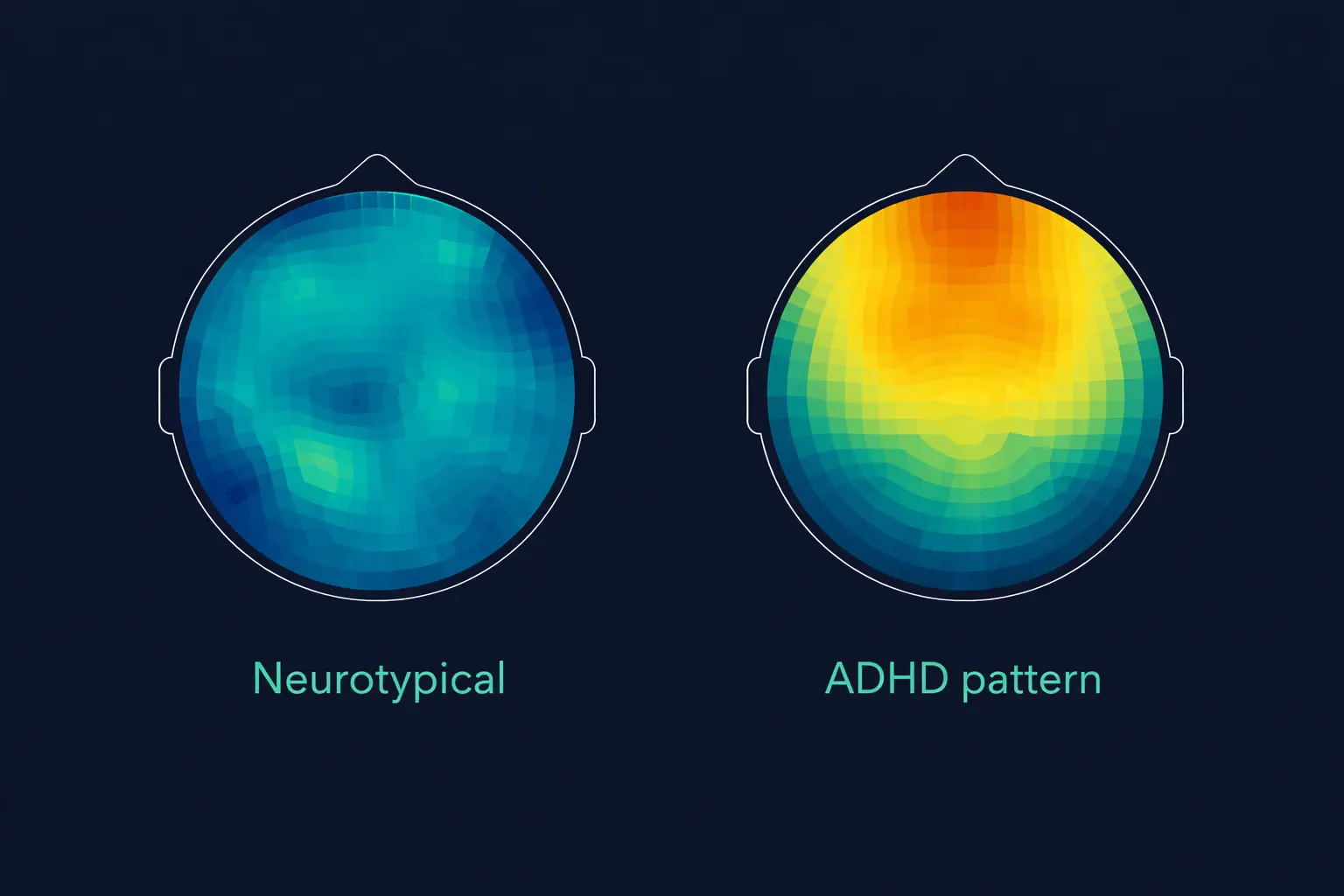
The default mode network (DMN) is a set of brain regions that become active when you are not focused on the external world — when you are daydreaming, reflecting, or mind-wandering. In neurotypical brains, the DMN deactivates when a task requires focus, allowing the attention network to take over.
In the ADHD brain, the DMN does not quiet down properly during tasks. It remains abnormally active, intruding on your attention and pulling your mind away from what you are trying to focus on. This is the neural basis of the experience of “zoning out” during meetings, conversations or reading — your default mode network is competing with your attention network, and frequently winning.
Understanding the DMN is essential because it explains one of the most frustrating ADHD experiences: you want to pay attention, you know the information is important, but your brain drifts away regardless of your intention. This is not a motivational failure — it is a failure of the neural switching mechanism that should suppress the DMN when task-focused networks activate. Stimulant medication helps by increasing dopamine in the prefrontal cortex, which strengthens the top-down suppression of the DMN during tasks. Many people describe the medication experience as “the noise in my head went quiet” — this is the DMN finally being suppressed when it should be. Exercise also improves DMN regulation, which is one reason why physical activity before demanding cognitive work can improve focus for 60–90 minutes afterwards.
Emotional regulation — why feelings hit harder
ADHD affects emotional regulation far more than most clinical descriptions suggest. The prefrontal cortex normally acts as a brake on the amygdala — the brain’s emotional alarm system. When the PFC is underactivated, emotional signals from the amygdala reach consciousness at full volume without being modulated.
This means:
- Frustration escalates faster and feels more intense than the situation warrants
- Excitement can be overwhelming — leading to impulsive decisions made in moments of enthusiasm
- Boredom is not just unpleasant — it can feel physically painful, driving restless behaviour and sensation-seeking
- Rejection triggers disproportionate pain — a phenomenon called Rejection Sensitive Dysphoria (RSD), which many adults with ADHD describe as one of the hardest aspects of the condition. RSD affects relationships, workplace interactions and self-esteem in profound ways that standard ADHD descriptions rarely capture
A 2025 paper in the Journal of Innovations in Medical Research described this as “impaired prefrontal–limbic communication, particularly between the amygdala and ventromedial prefrontal cortex, resulting in heightened reactivity and poor affective control.” Understanding that this is neurological — not a personal failing — is the first step toward managing it. Our emotional regulation strategies and relationship guide offer practical techniques.
The reward system — why motivation is context-dependent
The ADHD brain’s reward system shows reduced anticipatory signalling. In neurotypical brains, the reward pathway activates when a future reward is anticipated — “if I finish this report, I get to relax tonight.” In ADHD, this anticipatory signal is weaker, making delayed rewards less motivating.
This explains the paradox of ADHD motivation:
- Tasks with immediate, built-in rewards (video games, social media, interesting conversations) generate their own dopamine and engage the brain effortlessly
- Tasks with delayed or abstract rewards (filing taxes, writing reports, cleaning the house) do not generate sufficient dopamine to activate the prefrontal cortex
This is not laziness. It is a measurable difference in how the reward circuitry communicates with the prefrontal cortex. Understanding this changes how you approach motivation: instead of “try harder,” the solution is to build immediate rewards and external accountability into the tasks themselves. See our task initiation strategies.
How qEEG measures your brain activity
A quantitative electroencephalogram (qEEG) uses small sensors placed on the scalp to detect the electrical activity produced by your brain’s neurons. Unlike structural brain scans (MRI, CT) which photograph brain anatomy, a qEEG captures brain function in real time — what your brain is actually doing, moment by moment, while you concentrate, rest, or perform a task.
During your ADHD brain screening, we record from electrode positions Cz, Fz, F3 and F4 — sites that sit directly over the prefrontal cortex and central cortex. The recording captures the amplitude and frequency of your brainwaves, which we then decompose into frequency bands: delta (1–4 Hz, deep sleep), theta (4–8 Hz, daydreaming and rest), alpha (8–13 Hz, relaxed alertness) and beta (13–30 Hz, active concentration and focus).
The balance between these bands reveals how your brain is managing activation. In many people with ADHD, the prefrontal cortex produces too much theta (slow, rest-mode activity) and too little beta (fast, focus-mode activity) during tasks that require sustained attention. This theta/beta imbalance was recognised by the FDA in 2013 as a diagnostic aid for ADHD, and it is the primary biomarker measured in your screening.
Importantly, the qEEG does not diagnose ADHD — it provides objective neurophysiological evidence that complements clinical assessment. Your screening report shows your theta/beta ratio compared against age-matched normative data from our database of 311+ subjects, giving your result meaningful clinical context. This data is designed to strengthen a referral for formal NICE NG87 assessment, not replace it.
The three recording conditions in your screening each reveal different information: eyes-open resting captures baseline cortical arousal, eyes-closed resting shows how your brain transitions between states, and the Go/No-Go task measures sustained attention and impulse control under cognitive demand. Together, they provide a comprehensive picture of your brain’s functional profile that a meta-analysis of neuroimaging studies has shown to be reliably different in ADHD compared to neurotypical brains.
The theta/beta connection — what your screening measured
During your qEEG screening, we measured the theta/beta ratio (TBR) — the balance between slow-wave (theta) and fast-wave (beta) brain activity at the top of your head (electrode Cz).
Here is how it connects to everything above:
- Theta waves (4–8 Hz) are associated with the default mode network — daydreaming, internal reflection, disengagement from the external world
- Beta waves (13–30 Hz) are associated with active cortical engagement — focused attention, cognitive processing, prefrontal cortex activation
- An elevated TBR means more “rest mode” activity relative to “focus mode” activity — the prefrontal cortex is not reaching its optimal activation level
This cortical underarousal pattern is consistent with the dopamine and norepinephrine signalling differences described above. It also explains why stimulant medication can be effective — by increasing dopamine and norepinephrine in the PFC, medication helps shift the balance from theta-dominant to beta-dominant activity. A follow-up scan after starting medication can objectively demonstrate this shift.

Brain development — the 3-year delay
Longitudinal imaging studies have shown that the ADHD brain follows a delayed but normal developmental trajectory. Peak cortical thickness in the prefrontal cortex is reached approximately 3 years later than in neurotypical children — around age 10.5 in ADHD versus age 7.5 in typical development.
This delay is most pronounced in the regions responsible for attention control, planning and impulse regulation. It means that a 10-year-old with ADHD may have prefrontal maturity closer to that of a 7-year-old — explaining why expectations based on chronological age often feel impossible to meet.
The brain does eventually mature, which is why some ADHD symptoms reduce with age. However, the majority of adults retain clinically significant symptoms, and the executive function difficulties typically persist into adulthood even when hyperactivity diminishes.
How medication changes the brain
Stimulant medications like methylphenidate (Concerta, Medikinet) and lisdexamfetamine (Elvanse) work by increasing dopamine and norepinephrine availability in the prefrontal cortex. They do this by blocking the reuptake transporters that remove these neurotransmitters from the synapse, allowing them to remain active longer.
At therapeutic doses, research shows that stimulants:
- Preferentially affect the prefrontal cortex rather than reward pathways, which is why therapeutic doses reduce impulsivity rather than creating euphoria
- Normalise activation patterns — meta-analyses show medication reduces the abnormal under-activation in the frontostriatal and frontoparietal circuits that characterise ADHD
- Improve default mode network suppression — the DMN quiets down more effectively during focus tasks, reducing mind-wandering
- May normalise the theta/beta ratio — by increasing beta activity through enhanced prefrontal engagement
For a full guide to medication options, side effects and the titration process, see our ADHD medication guide. To objectively measure whether medication is changing your brain activity, consider a follow-up medication response scan.
Neuroplasticity — your brain can change
One of the most important findings in modern neuroscience is that the brain is not fixed. Neuroplasticity — the brain’s ability to reorganise and strengthen neural connections throughout life — means that the ADHD brain can and does change in response to treatment, environment and behaviour.
What changes the ADHD brain
- Medication. Stimulant medication does not just mask symptoms — research shows it normalises activation patterns in the prefrontal cortex and strengthens frontostriatal connectivity. A follow-up qEEG scan can demonstrate these changes objectively by showing shifts in your theta/beta ratio after treatment
- Exercise. Regular aerobic exercise increases BDNF (Brain-Derived Neurotrophic Factor), which supports the growth of new neural connections in the prefrontal cortex. Chronic exercise programmes of 12+ weeks produce lasting improvements in executive function that persist between sessions
- Sleep. Optimising sleep directly supports prefrontal cortex recovery and consolidation of learning. Even modest improvements in sleep quality can measurably improve attention, working memory and emotional regulation
- Cognitive strategies. External scaffolding — calendars, reminders, environmental design, habit stacking — does not just compensate for executive function deficits. Over time, consistently using these strategies strengthens the neural pathways associated with organised, goal-directed behaviour
- Therapy. Cognitive behavioural therapy adapted for ADHD targets the thinking patterns and beliefs that develop after years of undiagnosed ADHD — the self-criticism, the learned helplessness, the assumption that effort is futile. Changing these patterns creates measurable changes in brain activation during emotional processing tasks
The combination of medication, exercise, sleep optimisation and cognitive strategies produces compound benefits that exceed any single intervention alone. This is why a comprehensive approach to ADHD management is more effective than relying on medication as a sole treatment. Your brain is not broken and it never was. It is a brain with a different neurochemical profile, a different developmental trajectory, and a different set of strengths and challenges. With the right support, understanding and treatment, the ADHD brain — it is different, responds remarkably well to the right inputs. The evidence for this is not theoretical — it is measurable, objective and visible in your own brain data through qEEG screening and follow-up scans.
The ADHD brain in women
The neuroscience of ADHD does not differ fundamentally between men and women, but the expression of these brain differences varies significantly. Women with ADHD are more likely to present with inattentive symptoms — the quiet, internal manifestation of prefrontal underactivation — rather than the hyperactive-impulsive presentation that is more visible and more commonly identified.
Additionally, oestrogen directly modulates dopamine receptor sensitivity in the prefrontal cortex. This means the ADHD brain functions differently across the menstrual cycle, during pregnancy, and through menopause. When oestrogen is high, dopamine signalling improves and ADHD symptoms may lessen. When oestrogen drops, the prefrontal cortex loses hormonal support and symptoms worsen. This hormonal dimension of ADHD neuroscience is increasingly recognised by specialist clinicians but remains poorly understood in general practice.
Our screening for women page explains why objective brain data is particularly valuable for women whose ADHD symptoms may be masked by compensatory strategies and dismissed by clinicians unfamiliar with inattentive presentation.
ADHD and intelligence — they are not related
ADHD has nothing to do with intelligence. It affects the regulatory systems that direct cognitive abilities — not the abilities themselves. Many people with ADHD are highly creative, entrepreneurial, empathetic and capable of extraordinary focus on topics that engage them.
The difficulty is not thinking — it is directing thinking. Not capability — but consistency. Not intelligence — but regulation. This distinction matters because years of struggling with a brain that does not cooperate on demand can erode self-esteem and create a false narrative of being “lazy,” “stupid” or “not trying hard enough.”
Understanding the neuroscience dismantles that narrative. You are not failing — your brain is working with a different operating system. The right support — strategies, medication, workplace adjustments, and self-knowledge — can help you work with that operating system rather than against it.
Frequently asked questions
Yes. Brain imaging studies consistently show structural and functional differences in the prefrontal cortex, basal ganglia, cerebellum and default mode network. The ADHD brain follows a delayed developmental trajectory with peak cortical thickness reached approximately 3 years later than typical. ADHD is classified as a neurodevelopmental condition by the WHO, DSM-5 and NICE (NG87).
Interesting or rewarding tasks generate their own dopamine and norepinephrine, naturally engaging the prefrontal cortex and suppressing the default mode network. Boring tasks require the brain to generate neurochemical support internally — which is where the ADHD brain struggles. It is not willpower. It is a difference in how the brain mobilises its attentional resources.
The theta/beta ratio reflects the balance between “rest mode” and “focus mode” brain activity. An elevated TBR indicates cortical underarousal — the prefrontal cortex is not activating sufficiently during tasks. This is consistent with the dopamine signalling differences in ADHD and explains why stimulant medication can normalise brain activity.
Yes. The prefrontal cortex reaches peak thickness approximately 3 years later in ADHD. This means a child with ADHD may have executive function maturity closer to a child 2–3 years younger. Most adults retain significant symptoms even as the brain matures, particularly in executive function and emotional regulation.
Stimulant medications block dopamine and norepinephrine reuptake transporters, increasing availability of these neurotransmitters in the prefrontal cortex. This strengthens the PFC’s ability to regulate attention, suppress the default mode network, and maintain working memory. At therapeutic doses, the effect is preferentially in the PFC rather than reward pathways.